- Home
- Transforaminal Endoscopic Lumbar Discectomy for Large Central Herniated Disc Under Local Anesthetic in a Nonagenarian
Transforaminal Endoscopic Lumbar Discectomy for Large Central Herniated Disc Under Local Anesthetic in a Nonagenarian
Meng Huang, MD
Department of Neurosurgery, Houston Methodist Hospital, Houston, Texas, USA
Patient History / Exam
A 92-year-old male priestwas brought to the outpatient clinic with 3 weeks of acute onsetprogressive severe lower back pain radiating to both legs right worse than left all the way down to the feet but highly concentrated in the buttocks.He admitted to a baseline mild degree of chronic back pain that was normal to him, but otherwise did not have any prior history of lower back / radicular symptoms. He was otherwise healthy, and independent of his activities of daily living including driving and actively serving his congregation. At the time of presentation he was in severe discomfort, confined to the wheelchair, and his symptoms had not been responsive to a course of steroids and tramadol.
On physical exam, he appeared younger than chronological age by 20 years, butwas visibly uncomfortable due to severe pain. He did not have any confrontation strength deficits nor sensory deficits but had proximal pain limited weakness in the hip flexors.
ODI: 58% Disability and VAS: 6(Back)/9(RLE)/7(LLE)
Pre-Operative Imaging
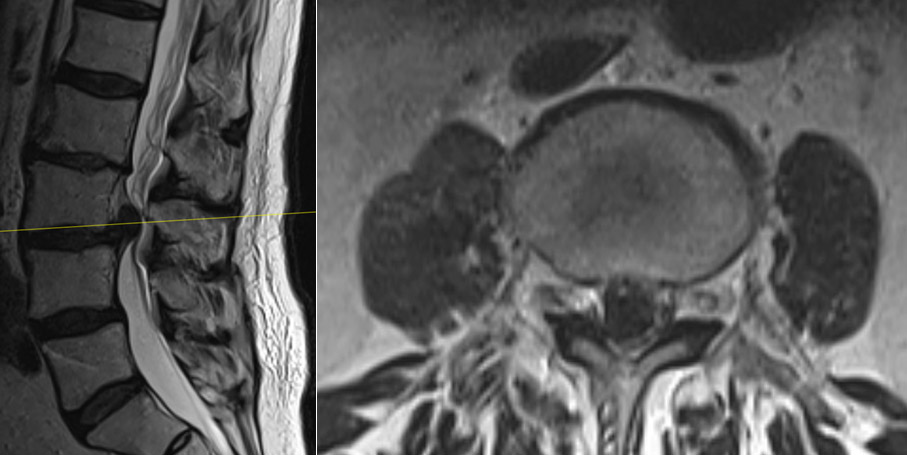
Figure 1. Non-contrast MRI of the lumbar spine revealed a large central herniated disc at L3-4. There was also a grade 1 spondylolisthesis at this level.
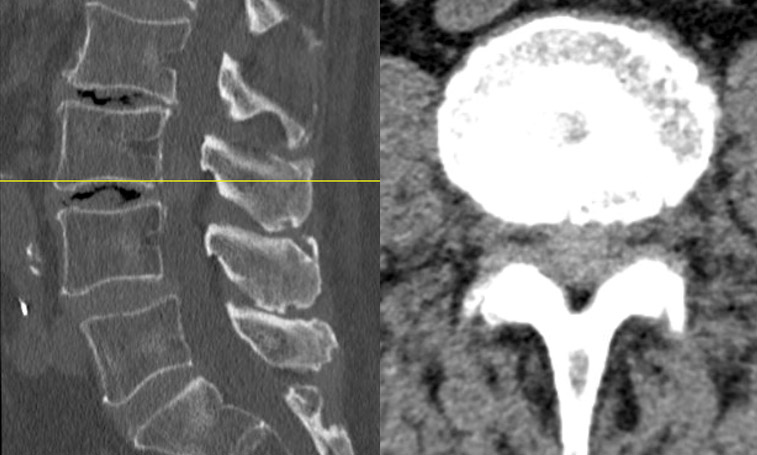
Figure 2. Non-contrast CT of the lumbar spine demonstrated that the herniation was not calcified. Intradiscal air/vacuum phenomena was present.
Diagnosis
Lumbar radiculopathy/neurogenic claudication secondary to L3-4 herniated central disc extrusion with severe thecal sac compression.
Treatment
Given the high ODI and sharp decline in his ability to accomplish ADLs while living alone, surgical intervention was warranted. Given his advanced age and preserved cognitive status, avoiding general anesthesia was preferred.He underwent an outpatient uniportalright transforaminal endoscopic discectomy under local anesthetic without complication.
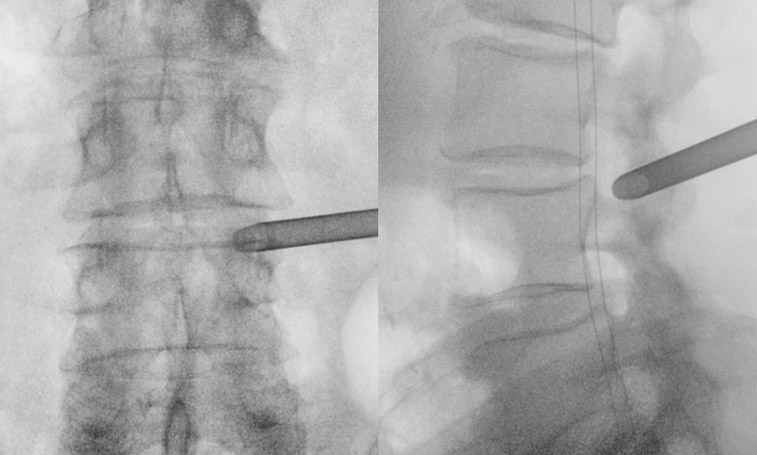
Figure 4. Intra-operative AP fluoroscopy image demonstrating localization and docking in the right L3-4 foramen. Lateral image showing docking caudal and dorsal in the safest part of kambin’s triangle.
Figure 5. Video demonstration of case.
Outcome
The patient experienced immediate and dramatic improvement in his symptoms. He took no pain medication whatsoever after surgery and was home within a few hours. At his 2week post-operative visit, he had sustained complete resolution of his preop pain VAS 2(Back)/0/0 and ODI 17%. At his 4 month post-operative visit, he had sustained complete resolution of his preop pain VAS 1(Back)/0/0 and ODI 15%.
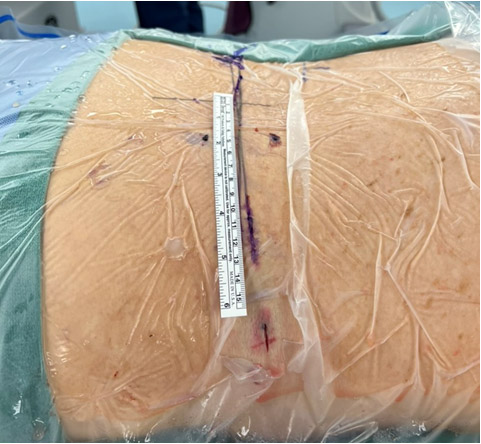
Figure 6. Photograph of incision/approach (Head to right, feet to left).
Discussion
Central large lumbar disc extrusions can sometimes require extensive laminectomy to resect. This could be morbid and destabilizing especially in an elderly patient who also has intradiscal air and spondylolisthesis.A transforaminal approach allowed us to access the ventral pathology directly without needing any iatrogenic disruption of the posterior elements. Furthermore, this approach allowed for surgery to be accomplished with local anesthetic rather than general anesthesia, which confers the advantage of reducing perioperative cognitive and cardiopulmonary risks in a nonagenarian.