Lumbar Spinal Deformity with Neuroforaminal Stenosis
Alex Whiting, MD
Juan Uribe, MD
Barrow Neurological Institute
History
63 year/o male with a history of severe back and leg pain. The patient described his pain as 50% leg pain and 50% back pain. He had tried multiple rounds of conservative treatment with no response. Having to deal with this sort of pain must be a struggle for anyone. People try many ways to reduce the pain. From visiting a chiropractor, doing regular exercises to even using something like this Plus CBD oil coupon to buy CBD products (as this is said to help reduce pains). But if it continues, getting medical advice is always best. In some cases, using products and techniques to reduce the pain is harmless due to the back problems disappearing on their own. However, in other cases, your back can only deteriorate more, especially with conditions like stenosis. These need attention immediately to start realigning your spine with treatments like endoscopic spine surgery.
Examination
The patient was neurologically intact.
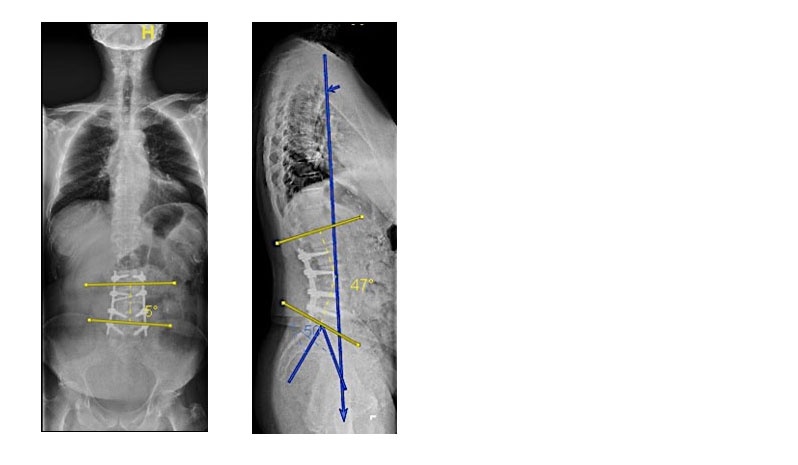
Pre-op. PL: 500 LL: 350 PT: 300 SVA: +6cm
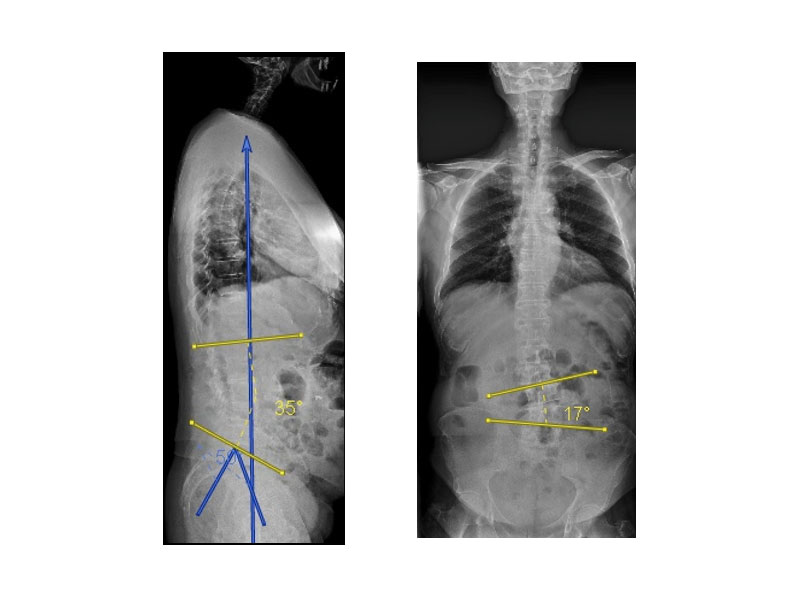
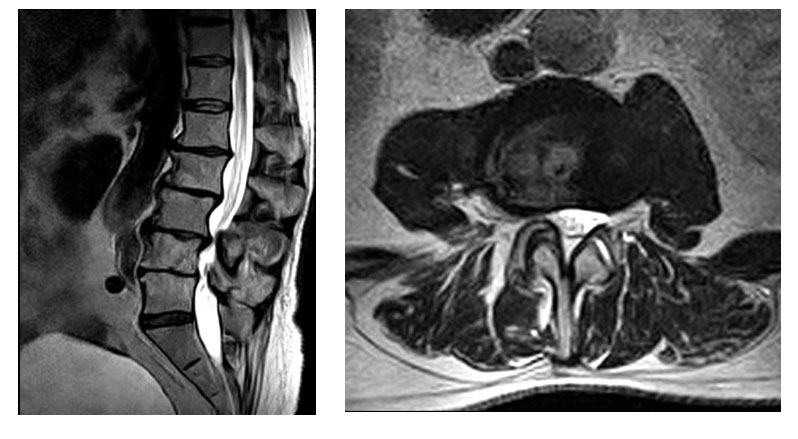
Pre-op MRI
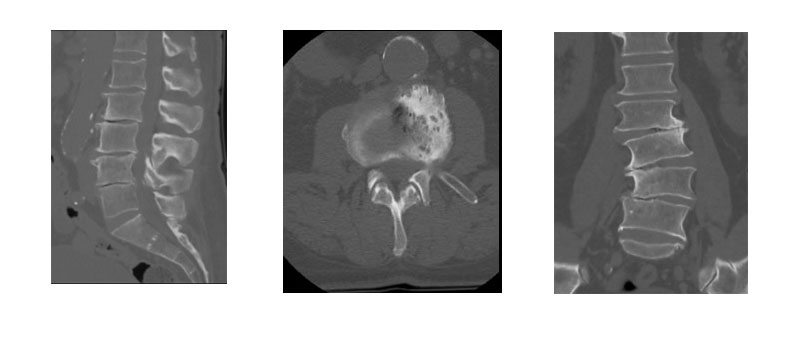
Pre-op CT
Diagnosis
Lumbar spinal deformity with neuroforaminal stenosis.
Treatment
The goal of surgery was to reduce the patient’s coronal deformity, perform indirect decompression of the patient’s neuroforaminal stenosis, and to provide appropriate lordosis in a minimally invasive fashion.
Stage 1: L2-L5 lateral lumbar interbody fusion with L3-L4 anterior column release.
Stage 2: Posterior percutaneous L2-L5 pedicle screw fixation with the use of a computer-assisted rod bending device.
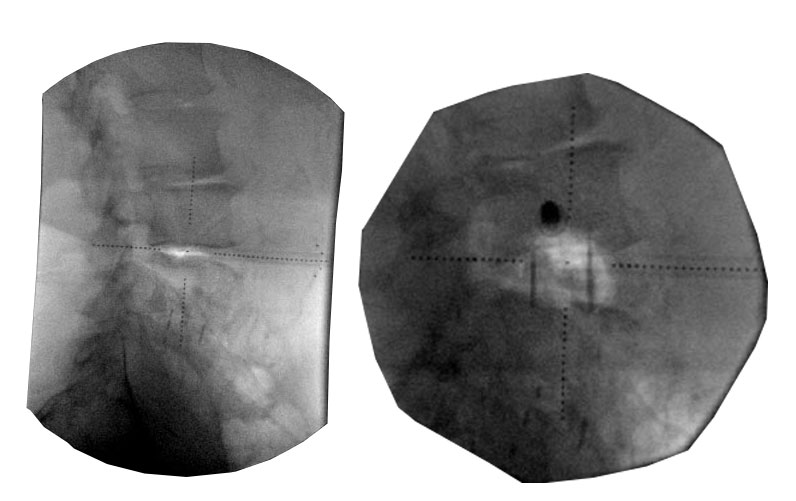
Stage 1:
Stage 2:
Intra-operative fluoroscopic images demonstrating increase in lordosis with anterior column release and hyper-lordotic graft at L3-4
Outcome
The patient had a significant and successful deformity correction with minimal soft tissue disruption and estimated blood loss of less than 200 cc.
The patient was discharged home 2 days after surgery, and demonstrated significant long-term reduction in her pre-operative pain.
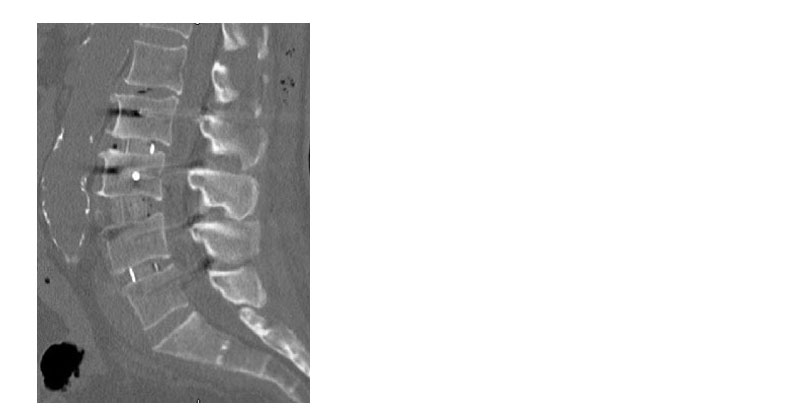
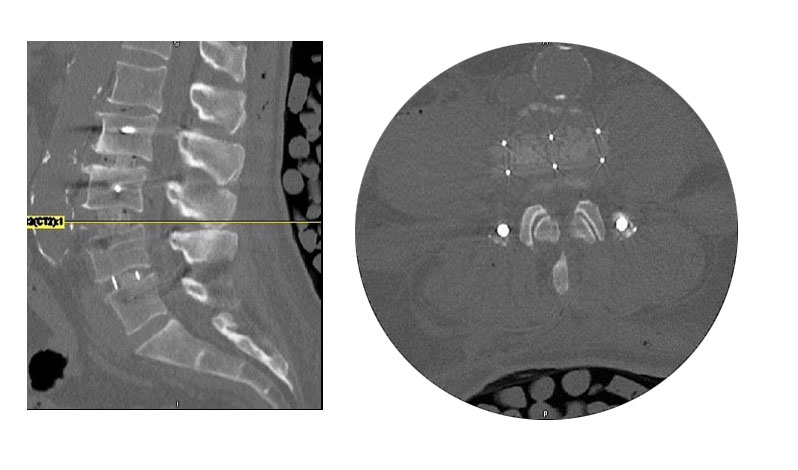
Post-operative CT scan demonstrating L3-L4 interbody placement
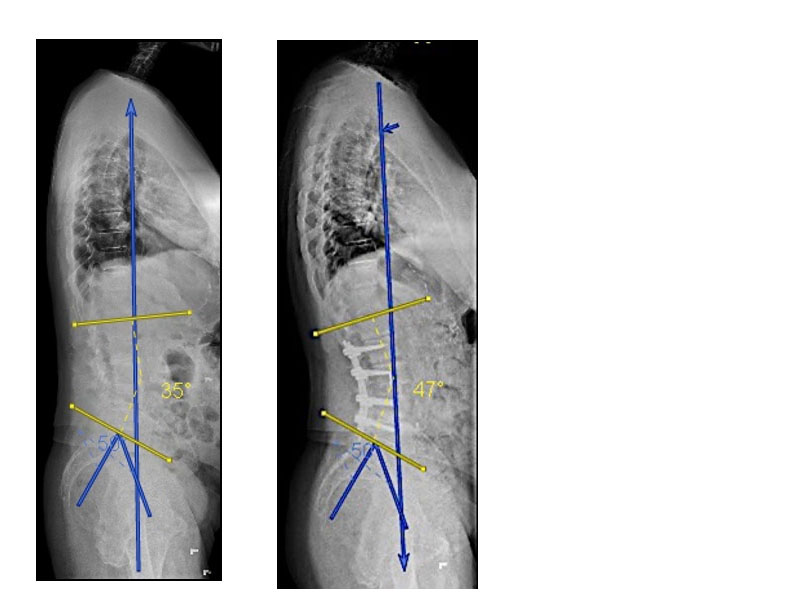
Pre and Post Op
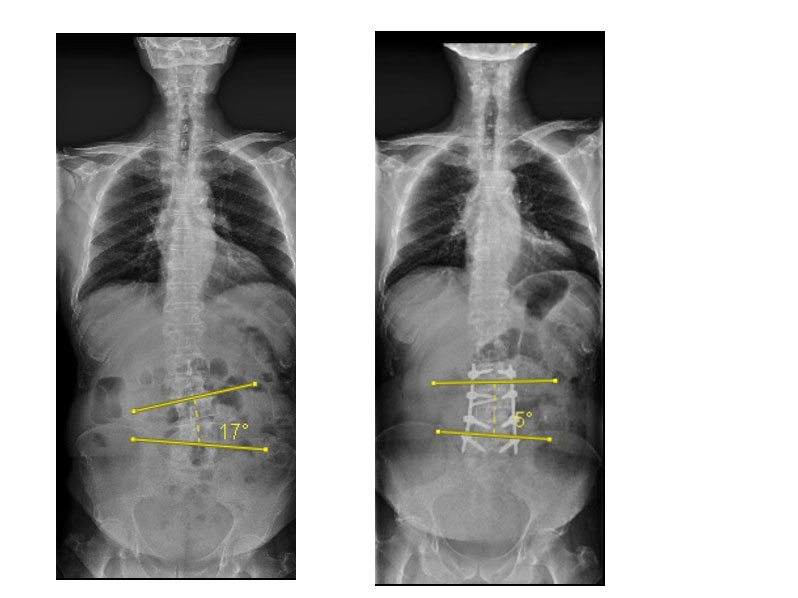
Pre-op: PL: 500 LL: 350 PT: 300 SVA: +6cm Post-op: PL: 500 LL: 470 PT: 250 SVA: +5 cm
Discussion
By performing a L2-L5 lateral interbody fusion, we were able to perform indirect decompression on the foramina at these levels, while also correcting the patient’s coronal deformity. An anterior column release at L3-L4 provided enough lordosis to correct the patient’s mismatch.
Use of computer-assisted rod bending allowed us to pass an appropriately contoured rod percutaneously without difficulty.
All of this was performed with minimal soft tissue dissection and minimal blood loss.