MIS Lateral Interbody with Posterior Instrumented Fusion and High BMI
Dr. Elizabeth Yu
Dr. Kathryn Jurenovich
Patient a 40 y.o. female presented with low back and bilateral leg pain. She previously worked cleaning houses. She has chronic back pain but worsened over the past six months and could hardly walk secondary to pain. The pain radiated from the back to the buttocks and into the lateral leg and foot. Her pain was worst with extension and standing up straight and better leaning forward. She had start up pain. She has trialed spinal ESI with improvement of her leg pain, but this returned. She was taking suboxone chronically for a history of IVDU, managed by pain management, as well as Tizanidine, Mobic, and Gabapentin.
She denied weakness or bladder/bowel complaints. No difficulty with hand dexterity. She did not have a history of previous spine surgery or injections. Her review of systems was noncontributory. Her BMI was 48.82. Pertinent past medical history included anxiety, depression, pseudo tumor cerebri, and PTSD. Past surgical history included cesarean section, cholecystectomy, and VP shunt.
On physical examination, she had an antalgic gait and unstable tandem gait. She had pain with lumbar extension and positive straight leg raises bilaterally. She had full strength in her bilateral lower extremities.
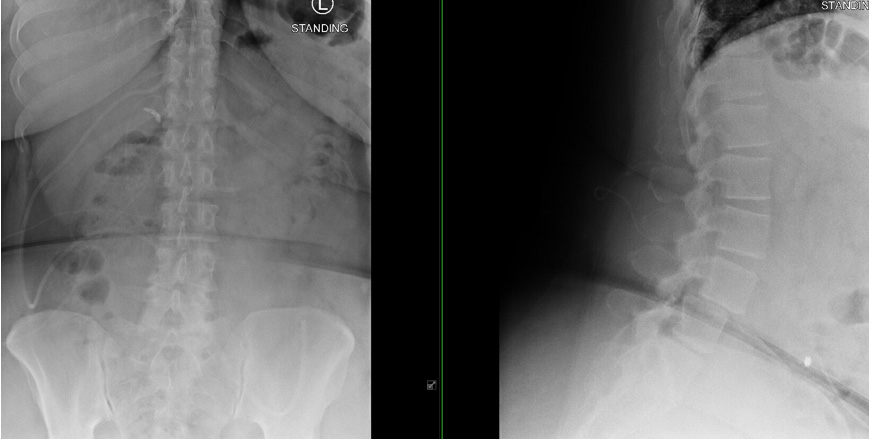
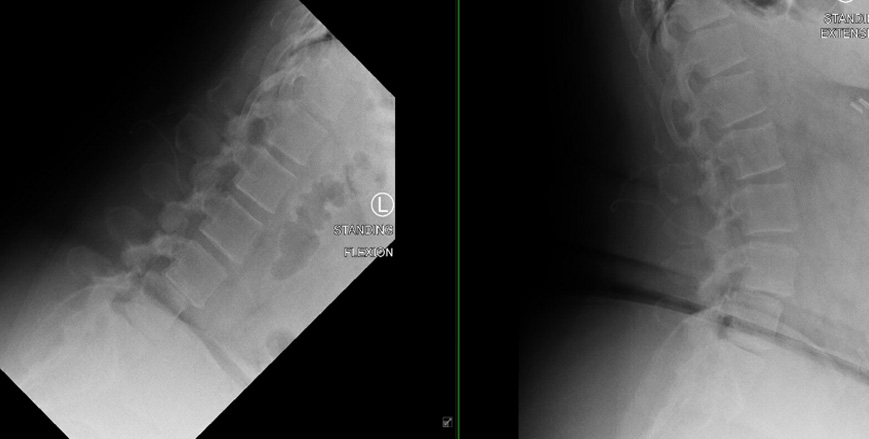
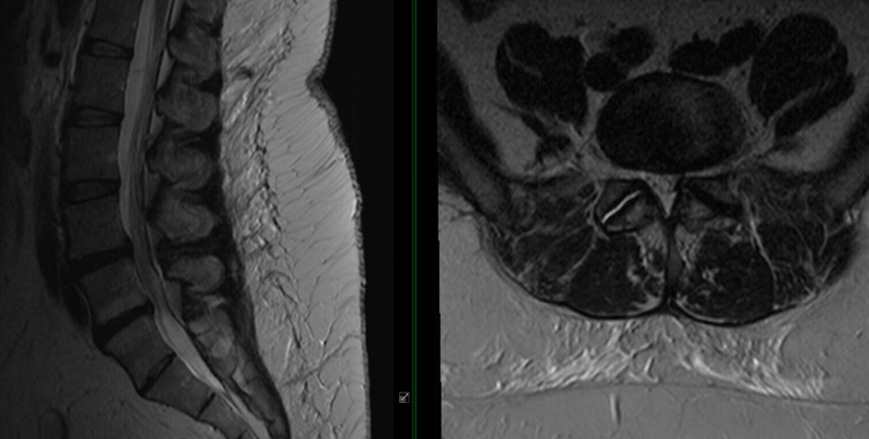
Her Xray demonstrated diffuse spondylosis with a hypermobile L4-5 anterolisthesis. Her MRI diffuse spondylosis with L4-5 anterolisthesis with moderate central stenosis at L4-5.
She had exhausted all conservative/nonoperative treatment measures and therefore recommend surgical intervention, to include L4-5 lateral interbody fusion, posterior L4-5 instrumented fusion, allograft and autograft.
She underwent a stage I anterior lumbar inter body fusion via a transpsoas approach L4-L5, and then had a stage II percutaneous L4-5 instrumented fusion. Neuromonitoring, allograft, fluoroscopy, and navigation were all used.
The procedure had no intraoperative complications. During her post-operative stay she was weight bearing as tolerated. IV antibiotics were continued for 24 hrs. Anticoagulation was started 24 hrs after postoperatively. PT/OT was initiated, and the chronic pain team was consulted.