Placement of MIS TLIF Cage Under Navigation
Alexander J Schupper, MD
Jeremy M Steinberger, MD
History
48 y/o female with past medical history of hypertension and low back pain, and a past surgical history of a L4-5 microdiscectomy in 2011 and a L3-4 microdiscectomy in 2017, who presented with three years of progressively worsening low back pain and proximal right lower extremity radiculopathy. She also reported associate numbness in her proximal right lower extremity. She had failed conservative treatments including pain medication and epidural steroid injections, as well as physical therapy.
Examination
Upon physical examination, the patient had full motor strength in all upper and lower extremity muscle groups. On sensory testing, the patient admitted having decreased anterolateral proximal thigh sensation on the right side.
Imaging
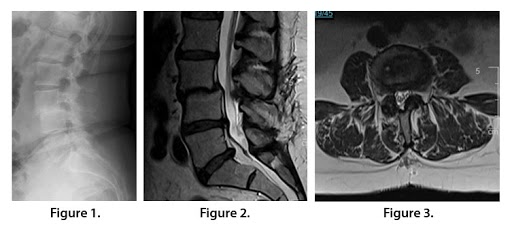
Sagittal plain films revealed disc space collapse at L3-4 (Fig. 1). MRI T2W sagittal (Fig. 2) and axial images (Fig. 3) revealed L3-4 spondylolisthesis with neuroforaminal stenosis, compression of the L3 and L4 nerve roots, and disk herniations at L4-5 and L5-S1.
Diagnosis
48 y/o female with L3-4 neuroforaminal stenosis and spondylolisthesis.
Treatment
Goal: Decompress the L3 and L4 nerve roots.
Challenge: Perform a minimally invasive transforaminal lumbar interbody fusion on a level with a collapsed disk.
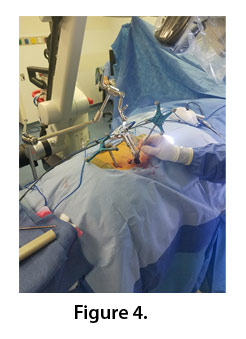
Selected surgical option: Minimally invasive transforaminal lumbar interbody fusion (TLIF) at L3-L4 with navigation (Fig. 4). Intraoperative visual guidance was utilized to help navigate the cage in the compressed disk space. The approach was gained through a 22 mm by 6 mm tube and performed using microscopic magnification. The L3 and L4 pedicle screws (6.5×40 mm) were placed under navigation, followed by a 7 height, expandable to 11, 10 width, 23 length mm cage placement with 13 degrees of lordosis.
Outcome
The patient underwent uncomplicated surgery. She remained neurologically intact postoperatively and reported minima6.5×40 x 4
l radicular symptoms at 3 months postop.
Discussion
Lumbar disc collapse following a lumbar laminectomy is not uncommon. As the disc space collapses, exiting nerve roots may be compressed, leading to compression of traversing and exiting nerve roots. Symptoms from foraminal nerve root compression may include pain and radiculopathy.
There are multiple treatment modalities for alleviating symptoms from nerve compression in the lumbar spine. Surgical options include direct and indirect decompression of affected nerve roots. Surgery may be performed in an open fashion, or in this case, minimally invasive. The patient in this case did not require central decompression, and therefore a minimally invasive approach to a transforaminal lumbar interbody fusion was performed.
The major challenge in this case was placing an interbody cage into a collapsed disc space through a minimally invasive approach. As an adjunct, navigation was employed to help localize the L3-L4 interspace for cage deployment through minimal exposure (Figure 4). The TLIF cage was able to be appropriately placed in the collapsed disk space, as well as the L3 and L4 pedicle screws (Figure 5), which allowed for improvement of lumbar lordosis, as well as indirect decompression of the affected nerve roots.

In a patient such as this case example, MIS TLIF can be a favorable option as a less invasive approach for nerve root decompression and restoration of spinal alignment. MIS may lead to faster recovery compared to open fusion, especially in a patient who has already received spine surgery in the same region.
Here, the authors favor the least invasive option where appropriate in the case of lumbar disc collapse and neuroforaminal stenosis.