Revision for 67-y/o With Proximal and Distal Junctional Kyphosis
Alex Whiting, MD
Juan Uribe, MD
Barrow Neurological Institute
History
A 67-year-old female presented with incapacitating back pain and severe sciatica pain. She had previously undergone a L1 – L5 interbody fusion with posterior percutaneous pedicle screw fixation with cement augmentation. She attempted conservative management with no response.
Examination
The patient was neurologically intact.
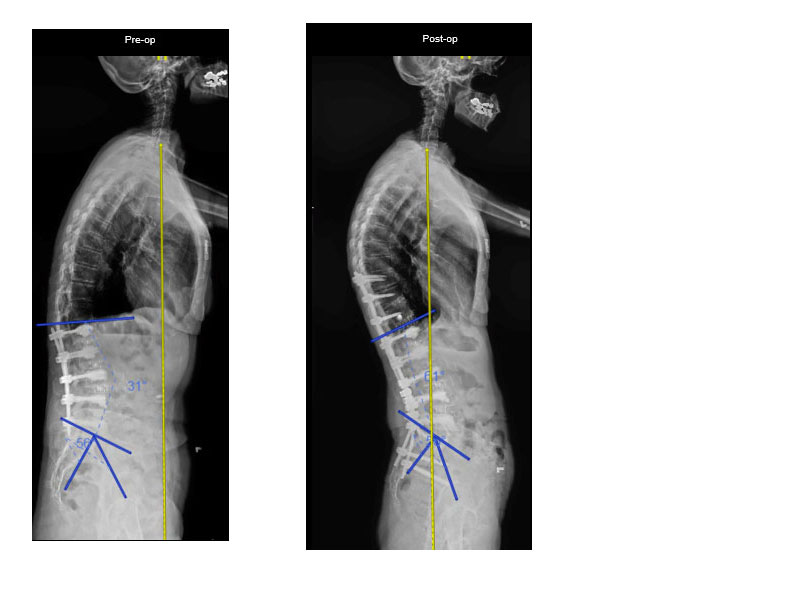
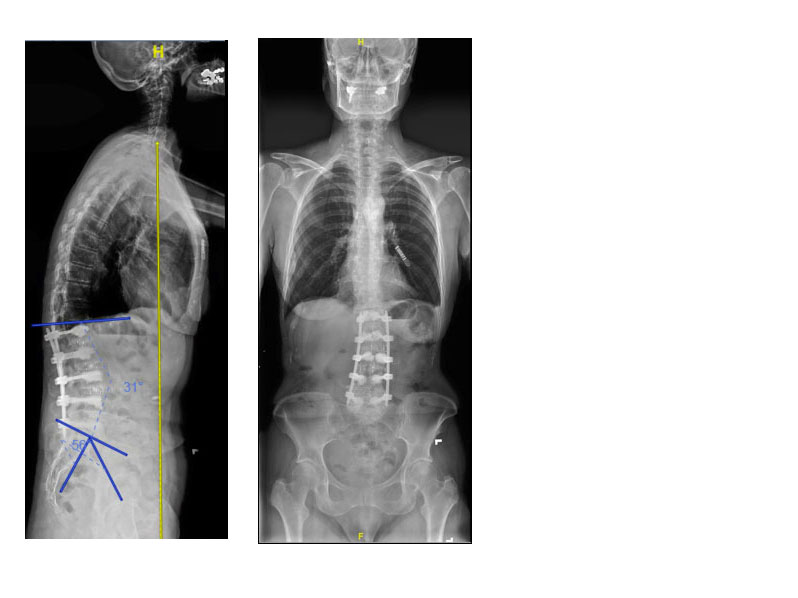
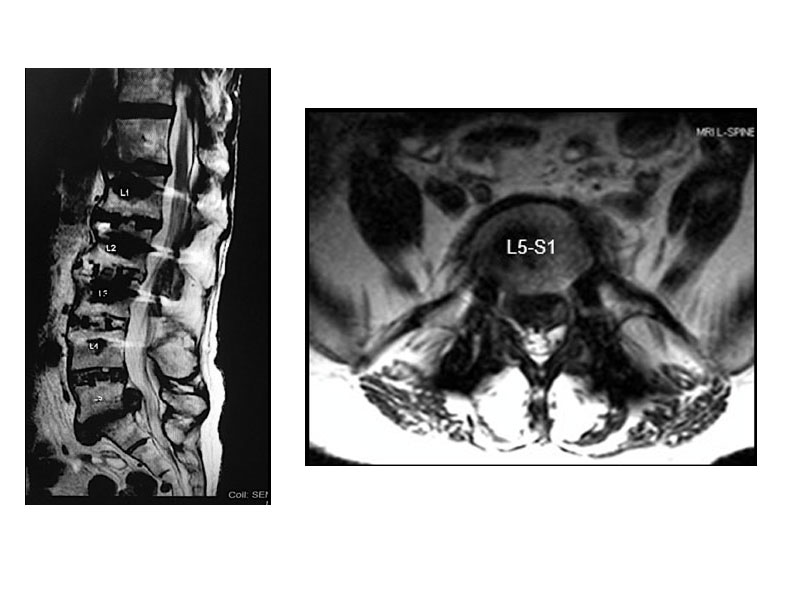
Pre-operative imaging
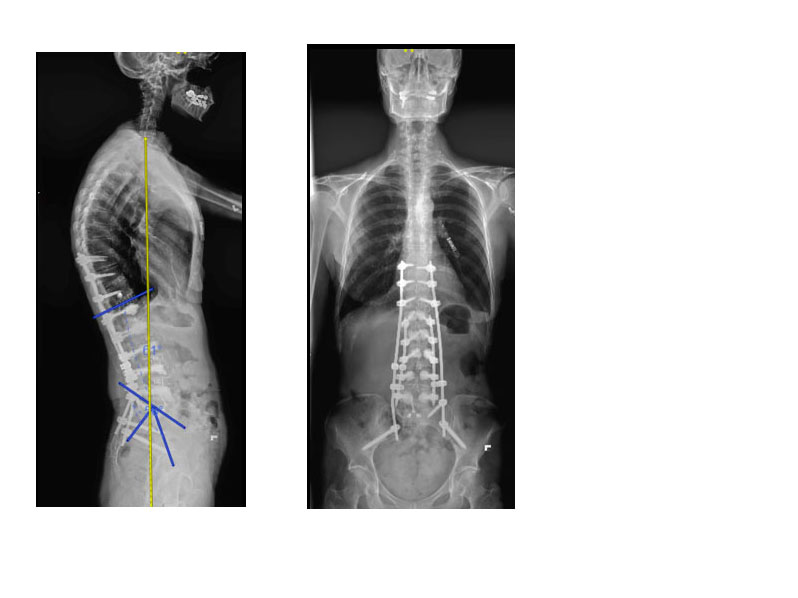
Imaging demonstrated proximal junctional kyphosis and distal junctional kyphosis at T12-L1 and L5-S1, with a large herniated disc at L5-S1.
Diagnosis
Proximal and distal junctional kyphosis.
LL: 310, PL: 560 , SVA: 11 cm
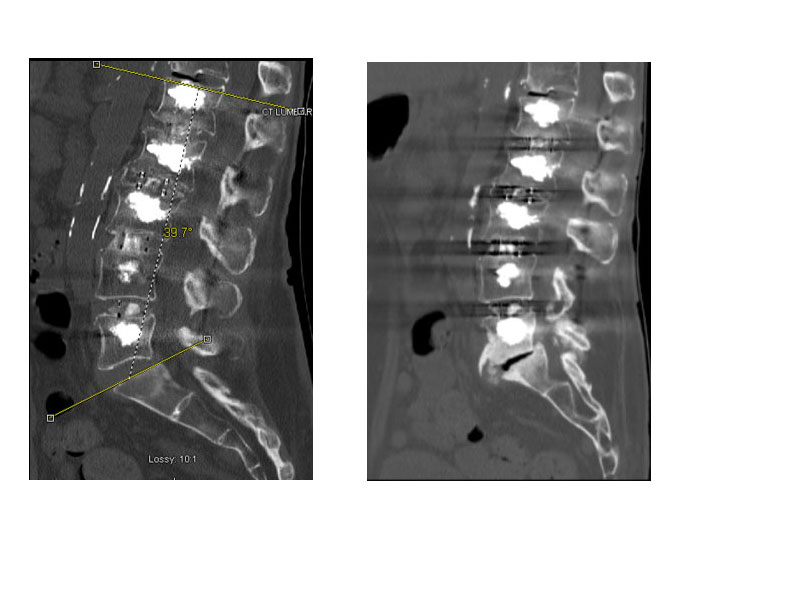
CT demonstrating vacuum phenomenon at L5-S1 and T12-L1
Treatment
The goal of the surgery was to restore appropriate sagittal balance and lumbar lordosis. To achieve this outcome we decided to do a 3-stage minimally invasive procedure with:
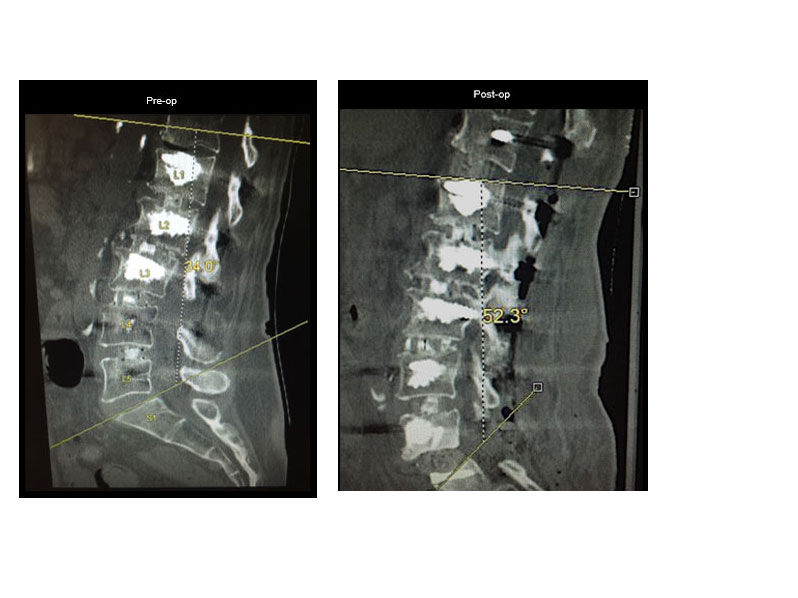
Stage 1: L5 – S1 anterior lumbar interbody fusion.
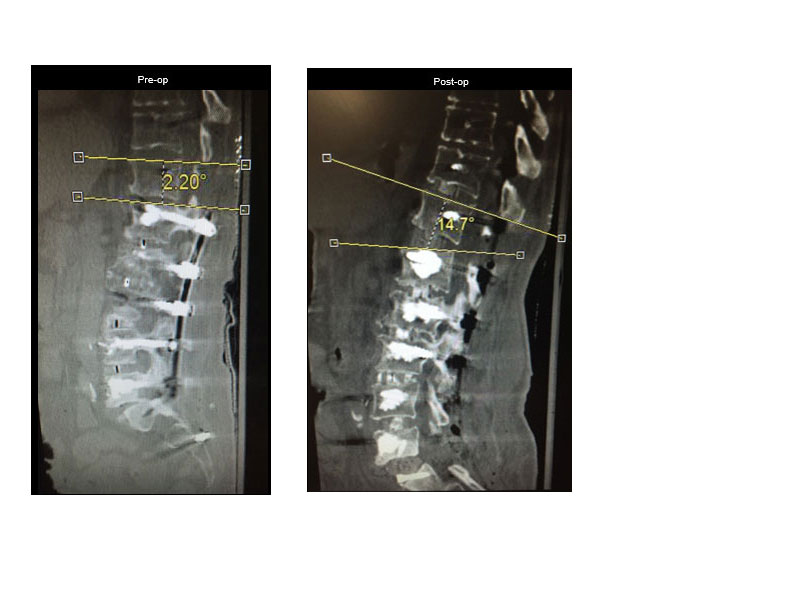
Stage 2: T11 – L1 lateral lumbar interbody fusion, with T12 – L1 anterior column release.
Stage 3: T10 – Ilium percutaneous pedicle screw fixation.
We placed percutaneous screws from T10-Ilium, skipping the previously fixated levels, and used a computer-assisted rod bending system to contour the rod to our desired parameters before passing it percutaneously.
Stage 1: L5-S1 anterior lumbar interbody fusion with anterior column release.
Stage 2: T11-L1 lateral interbody fusion with T12-L1 anterior column release.
Stage 3: Posterior percutaneous T10-Ilium fixation with the use of a computer-assisted rod bending device and connection to prior rod construct.
Outcome
By utilizing a minimally invasive approach, we were able to achieve the surgical goals, with minimal soft tissue disruption and an estimated blood loss of less than 400 cc.
By performing a L5-S1 anterior lumbar interbody fusion with a hyper-lordotic graft, we provided 18° of additional lordosis. We then performed a T11-L1 lateral lumbar interbody fusion with an anterior column release at T12-L1. This provided 12.5° of lordosis, as well as a large interbody graft for anterior fusion.
By placing a second rod percutaneously we were able to leave the prior fusion construct intact and link into the prior rod using connectors.

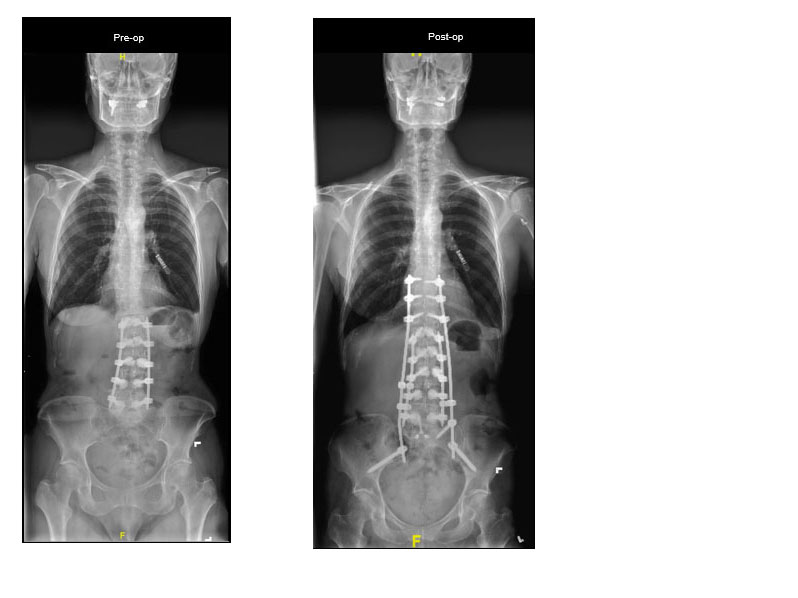
Pre-op: LL 310 PL: 560 SVA: 11 cm
Post-op: LL: 610 PL: 560 SVA: 2 cm