T12 Burst Fracture
Jackub Godzik, MD
Jay D. Turner, MD, PhD
Barrow Neurological Institute
Patient history / exam
38-year-old male presented after motor vehicle collision as an unrestrained passenger with acute back pain without radicular complaints. Patient was neurologically intact with tenderness to palpation over the posterior thoracolumbar spine.
Diagnosis
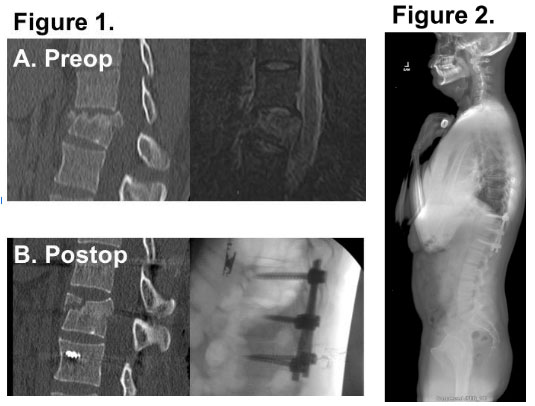
Imaging revealed a T12 burst fracture with suspected disruption of posterior ligamentous complex (TLICS 4). (Figure 1A)
Treatment
Nonoperative management with bracing versus surgical stabilization via open or minimally invasive techniques were discussed with the patient. We ultimately decided to proceed with percutaneous pedicle screw fixation from T11 to L1. Monoaxial screws were placed at T11 and L1 and ligamentotaxis used to reduce the fracture and correct the focal kyphosis. (Figure 1B)
Outcome
Excellent fracture reduction and realignment was achieved with minimal blood loss. Patient remained neurologically intact and was discharged home on postoperative day 2. He remained clinically stable at 3 months follow-up with stable instrumentation and alignment (Figure 2) and plan to explant the posterior instrumentation for motion preservation.
Discussion
Short segment percutaneous pedicle screw fixation without fusion is a viable option for treatment for of many thoracolumbar burst fractures. Excellent radiographic and clinical outcomes can be achieved with proper patient selection and surgical technique.